

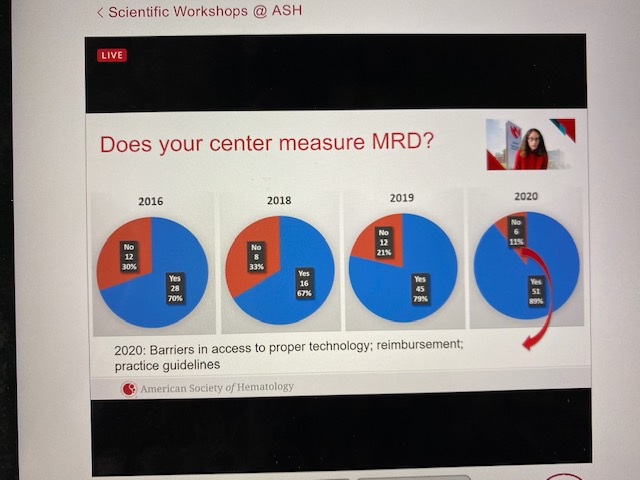
Minimal Residual Disease (-) (meaning no detectable disease) has become the agreed goal of most myeloma clinical trials. MRD (-) status is a predictor of good outcome. As we patients progress with treatment we want to know if we have reached MRD (-) or not, however it is defined, and by whichever method it is measured. Does your center measure MRD? At a Thursday pre-ASH BMT/CTN symposium, Dr. Sarah Holstein from the University of Nebraska Medical Center explained how this important lab evaluation has changed from 2016 to 2020, with 89% of reporting centers now checking this test for their patients.
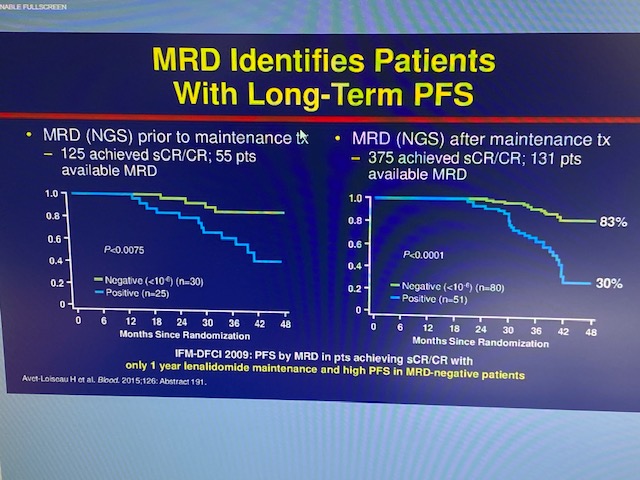
MRD was also discussed Friday morning at a satellite symposium. On Slide 2, Dr. Suzanne Lentzsch from Columbia Medical Center shows graphically that MRD identifies patients with long-term progression-free survival (PFS).
It checks a patient’s status at one point in time, but that status can change over time, either better or worse. Slide 3 shows the predictive trend of three or more measurements.
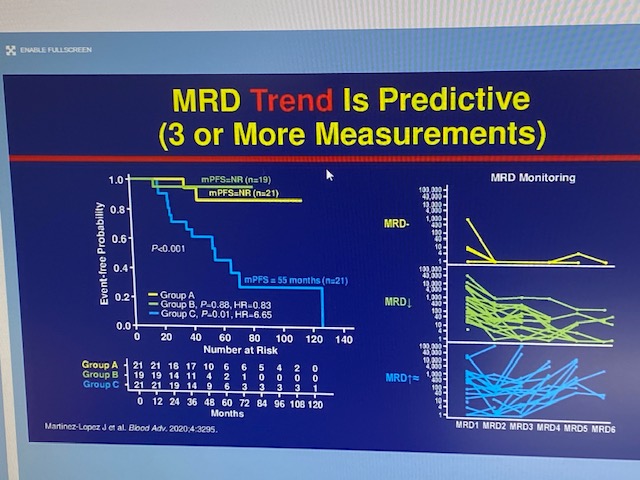
Notice the two yellow sets of lines of Groups A and B which trend downward over time. Compare them with the blue line of Group C, whose MRD status trended upward over time, and how their probability of relapse markedly changed, meaning their myeloma relapsed.
In Slide 4, she summarizes that MRD (-) is predictive of clinical risk of progression and prognosis.
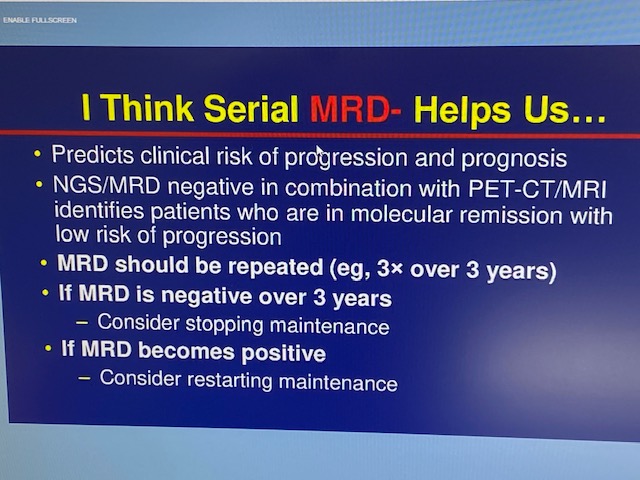
She feels that the test should be repeated at least three times over three years, and if it remains negative that consideration should be given to stopping maintenance therapy. Lastly, she also feels that if MRD becomes positive consideration should be given for resuming maintenance therapy, even if there are no clinical signs of myeloma relapse. All of this should be evaluated within the parameters of clinical trials.
Jim Omel MD