

There is no doubt that patients who continue maintenance Revlimid (lenalidomide) following autologous transplant do better than those who do not. Dr. Phil McCarthy showed unequivocally in CALGB 100104 (Revlimid vs placebo) that progression free survival (PFS) and overall survival (OS) are longer for patients taking maintenance Revlimid. Likewise, maintenance therapy extends PFS for patients not undergoing transplantation. While I am not questioning the value of maintenance therapy, I think it is important to periodically take critical looks at all aspects of myeloma treatments. That includes upfront autologous transplantation versus waiting for first relapse, intentionally deciding to forgo transplantation altogether, and the objectives of continuous maintenance therapy.
Maintenance therapy is administered for a prolonged period to maintain or improve response.
The goal is to eliminate any remaining minimal residual disease (MRD), or to maintain the absence of myeloma in MRD (-) disease. Maintenance therapy should reduce the risk of relapse and prolong PFS and OS. It should be convenient, safe and well-tolerated long term. Long-term maintenance therapy should not prevent the use, or reduce the efficacy, of other future treatments. Immunomodulatory drugs (IMiDs) are the backbone of long-term therapy, but proteasome inhibitors and monoclonal antibodies such as daratumumab or Ninlaro (ixazomib) are also used in selected patients.
Please consider Revlimid maintenance therapy and remember what Nina Shah of UCSF shared with us: “Therapy foREVer has its price.”
Most patients, not some, but most, get cytopenias while taking Revlimid. Grade 3 or 4 neutropenias occur at 59%. Grade 3 or 4 thrombocytopenias occur at 38% I took Revlimid maintenance for an extended period and contracted multiple URI infections. My white blood cell count chronically ranged from the high ones to mid-threes, rarely reaching 4. Since I was in stringent complete response (sCR), I made the decision to stop Revlimid and monitor for relapse. My myeloma did relapse, but it was four years later.
Another significant concern with long-term Revlimid maintenance is the potential for deep venous thrombosis (DVTs), and anticoagulation with aspirin or even something stronger is recommended. There are definite quality of life (QOL) factors to consider, one of the worst of which is fatigue, a general feeling of malaise or continuous tiredness. Diarrhea can definitely occur with Revlimid, and some members of my monthly myeloma support group refer to the drug as “Revli-poop” (sorry). Liver toxicity is listed as a potential complication, but I don’t know of anyone personally who has actually had transaminase elevations. Rash however is quite common. I had it. Just last week I told one of my members that her rash is most likely caused by the Revlimid she is taking and to talk to her doctor. Secondary primary malignancies (SPMs) can occur with Revlimid, but most experts feel this is the lasting effects of melphalan alkylator toxicity after transplantation. Lastly, a huge factor is cost. At >$10,000 per month, this drug is prohibitively expensive without insurance or third party or company assistance. Even if insurance coverage is excellent, consider the cost to the entire health care system of $10,000 per patient per month indefinitely.
The last slide points to work being done by many researchers, including a large currently enrolling SWOG trial, which hopes to identify patients who might not need indefinite maintenance.
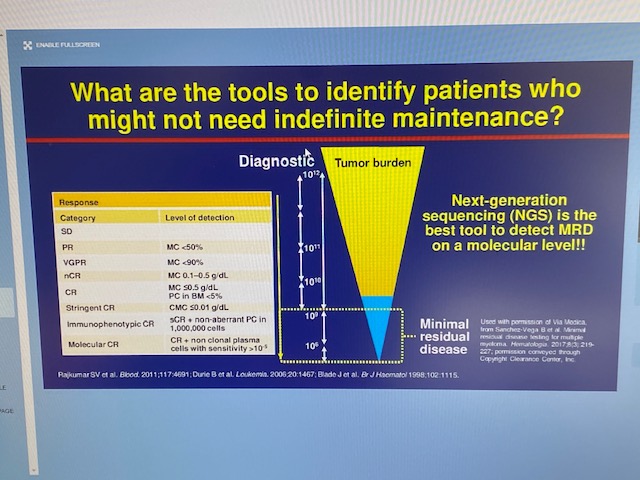
Multicolor next gen flow cytometry and NGS (next generation sequencing) can discover one myeloma cell hiding in one million normal bone marrow cells. Someday, we will have capability of checking MRD status with peripheral blood instead of painful marrow samples.
I end as I began, stating unequivocally that maintenance therapy extends PFS and OS for patients who can tolerate treatment. Many patients can’t tolerate continuous therapy however and their needs must be considered. Trials aimed to identify patients who can safely stop treatment with close monitoring for recurrence need our support. We as patients can help ourselves; and others like us, by agreeing to clinical trials which are appropriate to our myeloma condition.
Maintenance therapy is exceedingly helpful; but like all areas of myeloma treatment, it deserves reevaluation for each patient on an individual basis.
Jim Omel, MD